
UPDATE: Pre-budget hearing rallies!
Posted: February 1, 2016
(February 1, 2016)
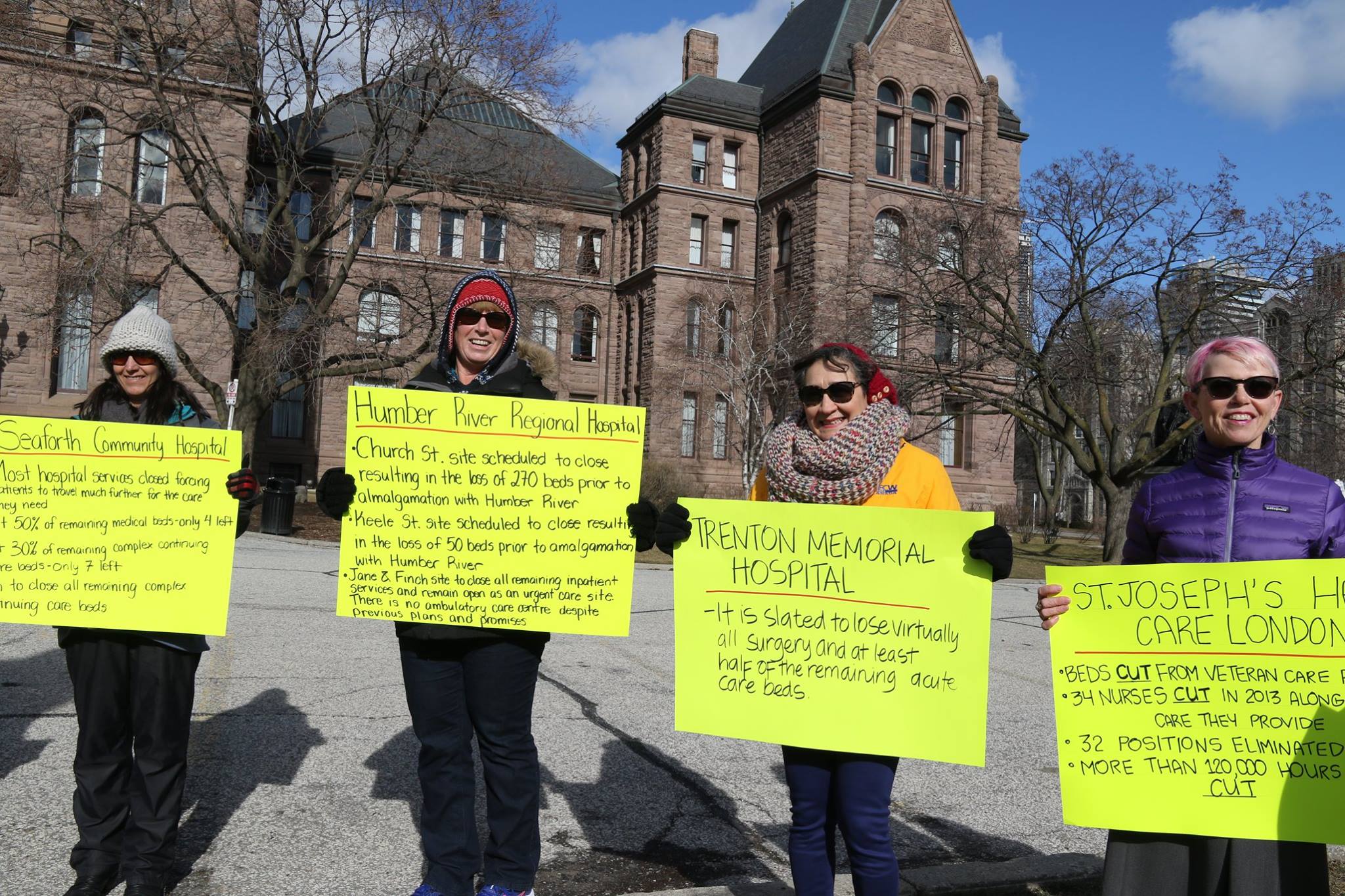
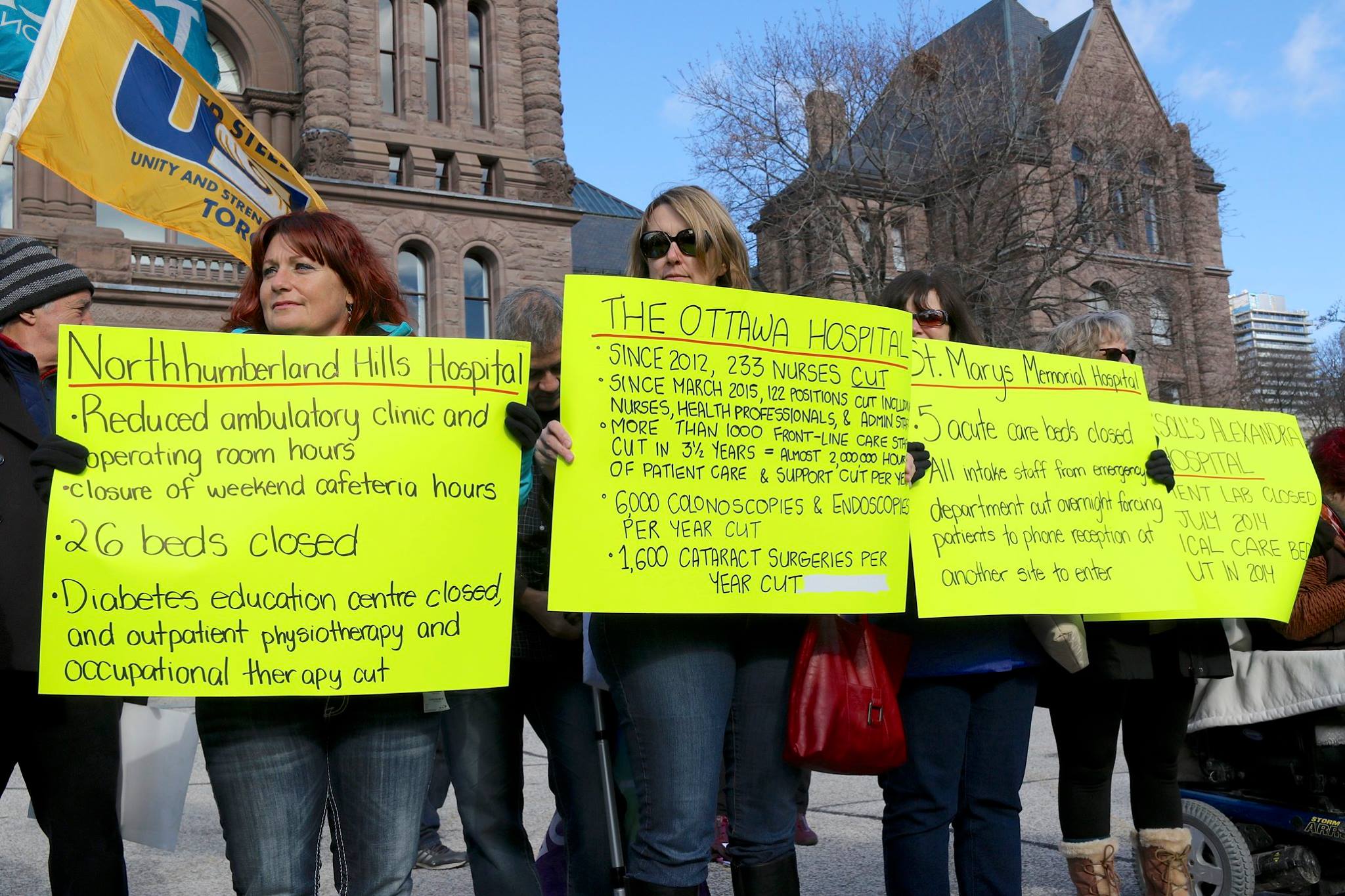
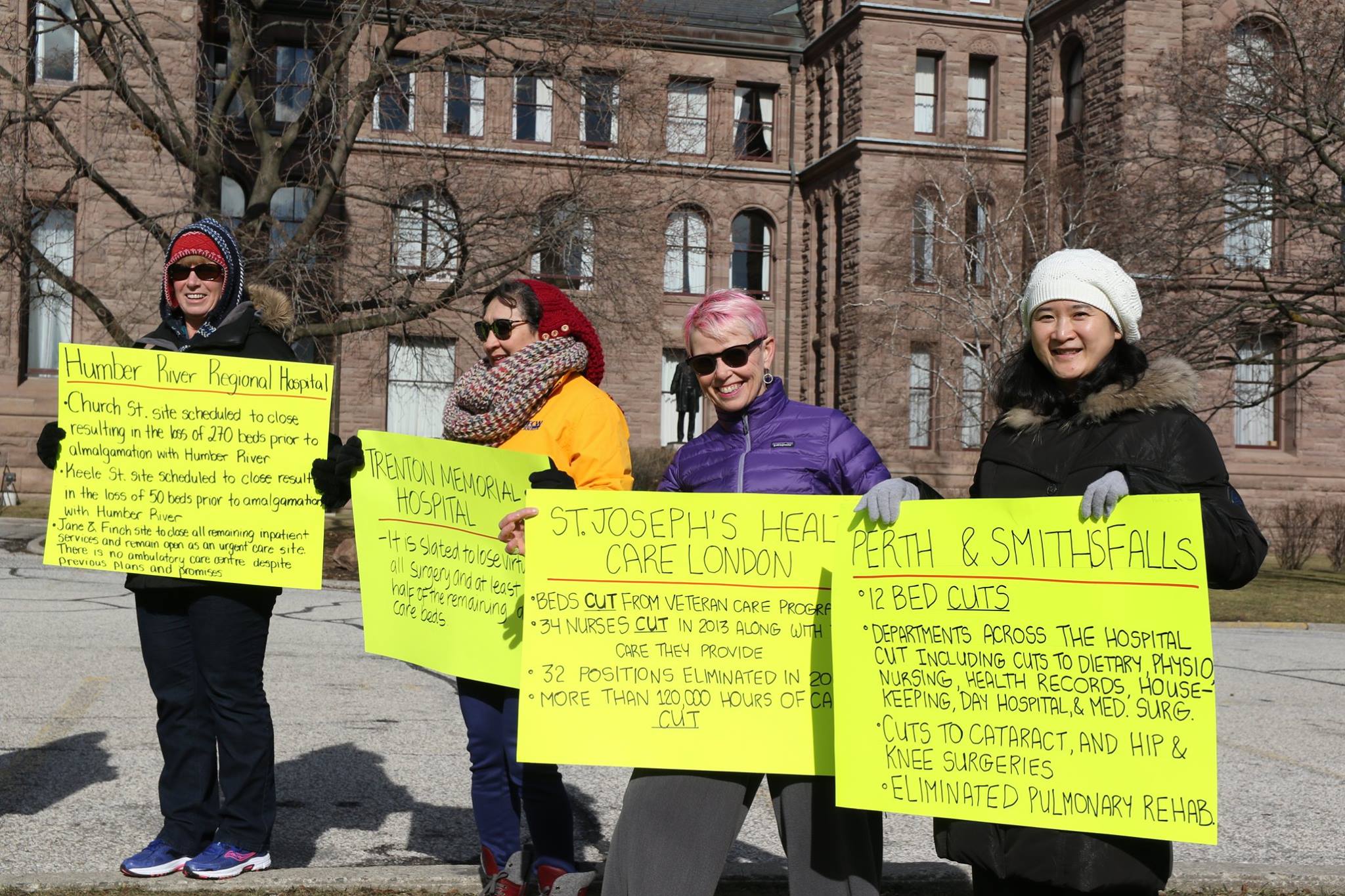
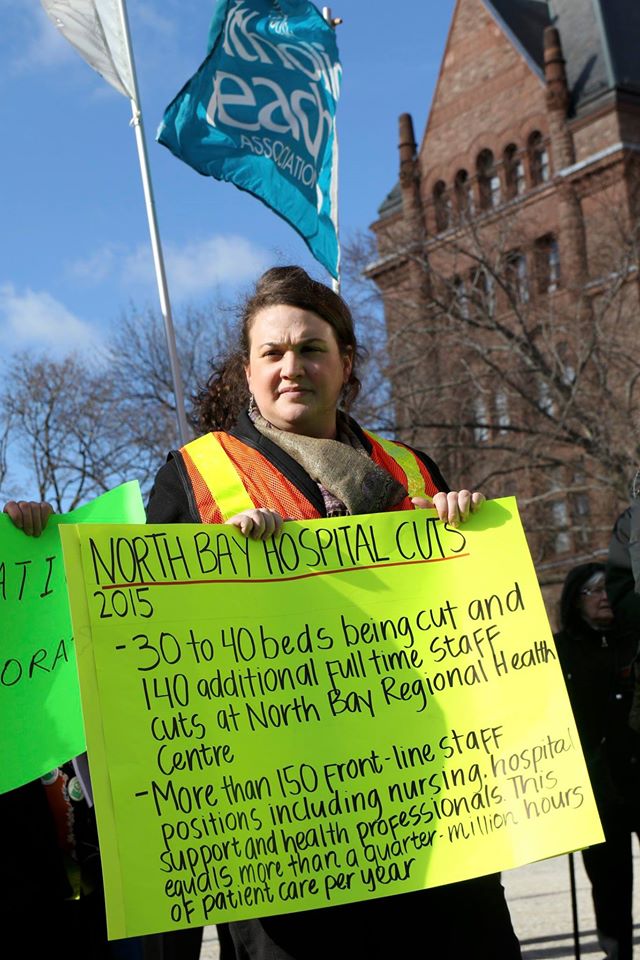
Ontario Health Coalition Executive Director presented to the Standing Committee on Finance and Economic Affairs at the Ontario Legislature this morning. Here is the Ontario Health Coalition’s submission with the most recent hospital spending, nursing levels (all nurse classifications), and hospital beds and overcrowding statistics. Please share with those who might be interested. Thank you to the hundreds of people who came out to our rally outside the hearings at the Ontario Legislature at noon.
Ontario Health Coalition Submission to the Standing Committee on Finance & Economic Affairs
Priority Recommendation: Stop Devastating Hospital Cuts & Restore Funding to Average of Other Provinces
Hospital global funding increases have been set below the rate of inflation since at least 2008. Since 2012/13 global hospital budget funding levels have been frozen. In sum, this means that global hospital budgets have been cut in real dollar terms (inflation-adjusted dollars) for 8 years in a row. This is the longest period of hospital cuts in Ontario’s history and there is no end in sight. The evidence shows that the hospital funding formula and austerity measures that have cut global hospital budgets in real dollar terms for almost a decade, have resulted in a dramatic reduction in needed services. By key measures, Ontario now ranks at the bottom of comparable jurisdictions in key measures of hospital care levels.
As a result, hospitals large and small in every geographic region of Ontario are cutting needed services. Hospitals are now at dangerous levels of overcrowding; staffing levels have dropped precipitously; and patients are suffering as they are forced to wait longer and drive further to access care and are discharged before they are stable.
A sampling of recent cuts:
- North Bay – 30 – 40 beds closing and 140 staff positions to be cut.
- Brockville – 17 Registered Nurses cut affecting departments across the hospital.
- London – up to 500 surgeries including hip, knee, gall bladder and others cancelled until next fiscal year due to inadequate funding of surgery budgets.
- Woodstock – hip, knee and other surgeries cancelled til next fiscal year.
- Trenton – virtually all surgeries cut and closed down along with half the remaining acute care beds.
- Minden – the hospital CEO is speculating openly about closing the Minden hospital.
- Niagara – five entire hospitals to be closed and replaced with one.
- Windsor — > 160 nurses and staff positions to be cut affecting departments across the hospital.
- Kitchener-Waterloo – 68 staff positions to be cut affecting departments across the hospital.
- Midland – at risk: birthing, cafeteria, OR closure 2 days per week, ICU beds to be cut, along with beds and other services.
The Ontario Health Coalition is deeply concerned about the cuts to our province’s public hospitals and has focused our pre-budget submission on one key recommendation:
Recommendation: The hospital cuts must be stopped immediately. Hospital funding must be restored to the average of the other provinces in Canada and funding must go to restoring and improving service levels to meet population need.
Ontario Ranks at the Bottom in Key Indicators of Hospital Care Levels
The evidence is indisputable that Ontario’s government has cut hospital care to the lowest levels of all provinces in Canada. As illustrated in Chart 1, Ontario has the fewest hospital beds left per capita of any province, and that number is declining. In 2008-09, Ontario had 2.5 hospital beds per 1000 population, according to Canadian Institute for Health Information (CIHI) data. Today that number has dropped to 2.3 hospital beds per 1000 population. The other provinces average 3.5 hospital beds per 1000 people. The difference of 1.2 beds per 1,000 population is vast. On an aggregate per capita basis Ontario now has 16,440 less hospital beds than the average. In fact, Ontario’s government has cut more than 18,000 hospital beds since 1990 and still the cuts are continuing.
Chart 1.
|
Hospital Beds Per 1000 (population) By Province 2013-14 |
|
|
Newfoundland & Labrador |
4.6 |
|
New Brunswick |
3.8 |
|
Saskatchewan |
3.6 |
|
Nova Scotia |
3.4 |
|
Manitoba |
3.3 |
|
PEI |
3.3 |
|
British Columbia |
3 |
|
Alberta |
2.8 |
|
Ontario |
2.3 |
|
Average other provinces |
3.5 |
Author’s calculations from: Canadian Institute for Health Information, Data Table: Hospital Beds Staffed and in Operation 2013-14. Population statistics from Canadian Institute for Health Information, National Health Expenditures Database 2015.
Not only has Ontario cut more hospital beds than any other province in Canada, we also now rank at the bottom of international data on hospital beds per population. Compared to 33 countries of the OECD, Ontario is third last in hospital beds per capita, followed only by Mexico and Turkey.
Chart 2.
|
OECD Hospital Beds Per 1000 Population 2013 |
||
|
Japan |
13.3 |
|
|
Korea |
11.0 |
|
|
Germany |
8.3 |
|
|
Austria |
7.7 |
|
|
Hungary |
7.0 |
|
|
Poland |
6.6 |
|
|
Czech Republic |
6.5 |
|
|
France |
6.3 |
|
|
Belgium |
6.3 |
|
|
Slovak Republic |
5.8 |
|
|
Luxembourg |
5.1 |
|
|
Estonia |
5.0 |
|
|
Finland |
4.9 |
|
|
Greece |
4.8 |
|
|
Switzerland |
4.7 |
|
|
Slovenia |
4.6 |
|
|
Norway |
3.9 |
|
|
Australia |
3.8 |
|
|
Italy |
3.4 |
|
|
Portugal |
3.4 |
|
|
Iceland |
3.2 |
|
|
3.1 |
||
|
Denmark |
3.1 |
|
|
Spain |
3.0 |
|
|
United States |
2.9 |
|
|
Ireland |
2.8 |
|
|
New Zealand |
2.8 |
|
|
United Kingdom |
2.8 |
|
|
Canada |
2.7 |
|
|
Turkey |
2.7 |
|
|
Sweden |
2.6 |
|
|
Ontario |
2.3 |
|
|
Chile |
2.2 |
|
|
Mexico |
1.6 |
|
|
OECD Average |
4.8 |
|
As hospital beds continue to be cut and closed down, nurses, health professionals and support staff have also been cut dramatically. Ontario has dropped to the bottom of the country in nurse to patient ratios. Data from the Canadian Institute for Health Information shows that Ontario now has the least hours of nursing care per hospital patient. Yet nurse staffing levels continue to be cut.
Chart 3.
|
Nursing Inpatient Services Total Worked Hours per Weighted Case |
|||||
|
2007-2008 |
2008-2009 |
2009-2010 |
2010-2011 |
2011-2012 |
|
|
NFLD |
52.2 |
53.26 |
54.48 |
55.9 |
52.9 |
|
PEI |
83.48 |
N/R |
62.19 |
62.46 |
61.66 |
|
N. S. |
56.79 |
57.34 |
U |
U |
54.95 |
|
N.B. |
54.98 |
55.46 |
56.26 |
57.29 |
58.13 |
|
Quebec |
49.73 |
50.06 |
50.82 |
50.73 |
52.47 |
|
Ontario |
44.98 |
44.76 |
43.71 |
42.81 |
42.88 |
|
Manitoba |
54.41 |
54.27 |
53.87 |
53.06 |
53.97 |
|
Saskatchewan |
49.37 |
51.42 |
51.28 |
52.95 |
54.18 |
|
Alberta |
54.12 |
54.65 |
54.52 |
54.24 |
54.36 |
|
B.C. |
44.24 |
45.27 |
45.03 |
45.87 |
46.27 |
|
NWT |
U |
83.05 |
88.51 |
69.48 |
N/R |
|
Yukon |
48.84 |
48.97 |
50.25 |
56.31 |
54.51 |
|
Weighted Average |
48.59 |
48.8 |
48.36 |
48.2 |
48.98 |
Source: Canadian Institute for Health Information, 2013.
Across Canada, patients receive 14.2 per cent more nursing care than do patients in Ontario’s hospitals. Chart 3 illustrates the growing gap between Ontario and the rest of Canada in nursing hours per patient (ie. per weighted case). In 2007 – 08 Ontario’s nurse staffing hours were 3.61 hours below the average of Canada per weighted case. By 2011-12, Ontario’s nurse staffing hours were 6.1 hours below the average of the country. That is a 69 per cent increase in the differential in just four years. As the hospital cuts have continued and escalated since 2011-12, we can expect that gap to be even wider when more recent data becomes available.
Eight Years of Real-Dollar Cuts Mean Ontario Has Dropped to the Bottom of the Country in Hospital Funding
The above data gives a statistical overview of some key indicators of hospital service levels in Ontario compared to other jurisdictions in Canada and internationally. The following section measures hospital funding compared to other provinces in Canada. As noted above, Ontario’s government has set global hospital operating funding increases below the rate of inflation for 8 consecutive years – the longest period of hospital cuts in our province’s history. For the last four years, hospital global funding has been frozen. In real dollar terms, Ontario is in its eighth year of hospital cuts. Today, by all measures, Ontario has dropped far below the other provinces in hospital funding.
Measured on a per capita basis, the most recent data from the Canadian Institute for Health Information National Health Expenditures Database shows that Ontario ranks second-last in hospital funding. For the last few years, Ontario and Quebec have traded places for lowest ranking in the country. We are significantly below the national average. In fact, Ontario’s government funds our public hospitals $501 less per person than the average of the other provinces.
Chart 4.
|
Public Hospital Funding Per Person, 2015 Current $ |
|
|
Newfoundland & Labrador |
$2,406 |
|
Alberta |
$2,245 |
|
Prince Edward Island |
$1,995 |
|
New Brunswick |
$1,971 |
|
Nova Scotia |
$1,907 |
|
Manitoba |
$1,818 |
|
British Columbia |
$1,797 |
|
Saskatchewan |
$1,761 |
|
Ontario |
$1,419 |
|
Quebec |
$1,382 |
|
Average of the other provinces |
$1,920 |
|
Difference between Ontario and the average of the other provinces |
Ontario funds hospitals at $501 per person |
Source: Author’s calculations from
CIHI, National Health Expenditures Database 2015Hospital spending per person is a clear comparison of how many resources our government is allocating to these services. To measure economic sustainability or affordability, GDP (which measures economic output) is used as the comparator. As measured as a percentage of provincial GDP, the results are the same. Ontario is second last in Canada, followed only by Saskatchewan which saw significant GDP growth in recent years. This measure shows that Ontario has room to improve hospital funding while keeping funding at sustainable levels, as long as funding goes to improving services.
Chart 5.
|
Public Hospital Funding as % of Provincial GDP 2015 |
|
|
PEI |
4.73 % |
|
New Brunswick |
4.45 % |
|
Nova Scotia |
4.31 % |
|
Newfoundland & Labrador |
3.82 % |
|
Manitoba |
3.59 % |
|
British Columbia |
3.35 % |
|
Quebec |
2.97 % |
|
Alberta |
2.67 % |
|
Ontario |
2.64 % |
|
Saskatchewan |
2.38 % |
|
Average of the other provinces |
3.59 % |
Source: Author’s calculations from
CIHI, National Health Expenditures Database 2015Sustainability can also be measured in terms of expenditure as a proportion of the provincial budget. In Ontario, hospital funding as a share of the provincial budget has been declining for decades. The most recent data show that we are third last among Canadian provinces for hospital spending as a proportion of total program spending. Again, the data show that we are considerably lower than the average of the other provinces and there is room to improve hospital funding to stop the cuts and restore service levels to meet population need.
Chart 6.
|
Public Hospital Funding as % of All Provincial Program Funding 2014 |
|
|
Nova Scotia |
20.72 % |
|
British Columbia |
19.44 % |
|
New Brunswick |
18.95 % |
|
Alberta |
18.91 % |
|
Newfoundland & Labrador |
18.61 % |
|
Manitoba |
17.94 % |
|
PEI |
17.56 % |
|
Ontario |
15.34 % |
|
Saskatchewan |
14.73 % |
|
Quebec |
11.16 % |
|
Average of other provinces |
17.56 % |
Source: Author’s calculations from
CIHI, National Health Expenditures Database 2015Hospital Overcrowding, Cuts and Early Discharges: Impact on Patients
|
Sampling of hospital bed occupancy rates (final quarter 2013) · Napanee/Lennox/Addington: 123% · Sault Ste Marie area: 114% · Toronto Hosp. for Sick Kids: 110% · Toronto Central: 110% · London Health Sciences Centre: 108% · Exeter South Huron: 106% · Burlington Joseph Brant: 106% · Hamilton Niagara Haldimand Brant: 106% · Niagara Health System: 104% · Windsor Hotel Dieu Grace: 101% · Erie St. Clair: 101% · Oakville Halton Health: 101% · Mississauga Halton: 101% · The Ottawa Hospital: 101% · Barry’s Bay St Francis: 101% · Thunder Bay Regional: 100% · Newmarket Southlake Reg.: 100% From Ministry of Health data accessed by Jonathan Sher, London Free Press. See: http://www.torontosun.com/2014/03/07/ont-health-ministry-data-on-hospital-overcrowding-riddled-with-errors |
Ontario has not conducted a hospital bed study to measure population need and assess how many hospital beds should be planned for more than fifteen years. To the extent that data is being used in planning at all, the numbers that are being used are two decades out of date. Instead of using an evidence-based planning approach, Ontario’s health policy has centred on constraining hospital budgets, cutting services and reducing patient length of stay. As a result, Ontario is suffering from a shortage of hospital beds and services that is negatively affecting patients’ access to care and safety.
Ontario’s hospital occupancy levels are extraordinarily high. According to Ministry of Health data, by 2010 there were, on average, 30,164 inpatients[1] in Ontario’s 30,810 hospital beds.[2] The provincial hospital bed occupancy rate is 97.8%, much higher than other jurisdictions. By comparison, the OECD reports an average occupancy rate for acute care beds of 75%.[3] In the United States, the average hospital occupancy rate is 68.2%.[4] Most often cited in the academic literature, a target hospital occupancy rate to reduce access blockages and improve outcomes is 85%.
The consequences of hospital overcrowding warrant public attention. Within hospitals, overcrowding is associated with serious quality of care issues. Overcrowded emergency departments do not have appropriate staffing ratios for critical care or intensive care patients who require intensive monitoring by specially trained staff. Across Europe, hospital occupancy rates have been cited as a determining factor in hospital-acquired infections (HAIs), and indeed Ontario has experienced repeated waves of Hospital Acquired Infection outbreaks. Cancelled surgeries and prolonged waits are associated with poorer health outcomes. Ontario’s extremely high occupancy poses a significant threat to patient safety and quality of care.
Emergency room overcrowding is epidemic among large and medium-sized community hospitals in Ontario, and a frequently noted factor in ER wait times is the unavailability of acute care beds.[5] In 2011, Ontario had, on average 592 patients waiting in emergency departments for admission to an inpatient bed. This represents almost 4% of Ontario’s total acute care beds.[6] A study by Ontario researchers has demonstrated that long waiting times increase the risk of death and hospital readmission for patients who have been discharged from the emergency department. This study, published in the British Medical Journal looked at 22 million patient visits to Ontario emergency departments over a five year period, and found that the risk of death and hospital readmission increased with the degree of overcrowding at the time the patient arrived in the emergency department. The authors estimate that if the average length of stay in the emergency department was an hour less, about 150 fewer Ontarians would die each year.[7]
Not only is there a problem getting into hospitals, there is also a serious issue of patients being discharged too early and without placement in home care and in long term care homes. The Advocacy Centre for the Elderly reports that they receive frequent complaints from patients who are subject to pressure tactics to move them out of hospitals. Hospital policies may include statements that if person refuses to pick from short lists of long term care facilities that are not of their choosing, or if the patient refuses to take first available bed, then will be charged a large per diem ranging from $600 a day to $1800 a day.[8] In many cases the charges levied against patients in an attempt to move them out of hospital are unlawful. In addition to reduced hospital beds and shorter lengths of stay for hospital patients, entire departments have been systematically cut from local hospitals. Outpatient rehabilitation, social work, laboratories and an array of outpatient services have been slashed. In many cases this care is moved far away from patients’ home communities, privatized and subject to new user fees, or simply inaccessible.
Consequences of Emergency Department Overcrowding
- Patient suffering, dissatisfaction and inconvenience
- Poor patient outcomes
- Increased morbidity and mortality
- Poor quality of care
- Contribution to infectious disease outbreaks
- Violence aimed at hospital staff and physicians
- Decreased physician and nursing productivity
- Deteriorating levels of service
- Increased risk of medical error
- Negative work environments
- Negative effects on teaching and research
|
Source: Physician Hospital Care Committee Report to the Ministry of Health and Long-Term Care, Ontario Medical Associaiton and Ontario Hospital Association Tripartite Committee, Improving Access to Emergency Care: Addressing System Issues, August 2006. |
Misalignment with Provincial Government Policy & Requirements of the Canada Health Act
Under the Canada Health Act, hospital and physician services are to be provided without financial barrier on equal terms and conditions to all Canadians. That means that the cost of illness and injury is to be shared by all Canadians, and care is to be provided through our public taxes so that people are not burdened when they are ill, injured or dying; when they are least able to pay. The fundamental principles of compassion and equity, of which Canadians are rightfully so proud, are embodied in this system of health care for all. The Canada Health Act was passed with unanimous support from all political parties in Parliament.
Provincial governments are expected to uphold the principles of Public Medicare for all, as enshrined in the Canada Health Act. But when public hospital services are cut, and services are offloaded from public hospitals, services are inequitable, subject to user fees, ad hoc and almost always privatized. Patients are faced with burgeoning user fees and costs that cause hardship and suffering, just when people are least able to bear them.
As hospital services have been cut, an increasing scope of care has been offloaded to private clinics. The Ontario Health Coalition has conducted repeated rounds of research aimed at determining how many private clinics are charging extra user fees to patients for medically necessary services. In our studies in 2008 and 2014, we found a significant number of private clinics that are charging patients hundreds to thousands of dollars on top of billing OHIP for services. In a significant number of cases, private clinics are charging patients for medically necessary services, in violation of the Canada Health Act. Increasingly, clinic operators are also using manipulative and confusing information to persuade patients that they will have poorer health outcomes if they do not pay hundreds or even thousands of dollars for their cataract surgeries and associated tests and assessments.
The evidence shows that ownership matters. Cuts to public hospital services are resulting in for-profit privatization of needed care, and private clinic operators are eroding the first principle of Public Medicare in Canada, that care must be provided equally, based on need not wealth.
Mission and Mandate
Our primary goal is to protect and improve our public health care system. We work to honour and strengthen the principles of the Canada Health Act. We are led by our shared commitment to core values of equality, democracy, social inclusion and social justice; and by the five principles of the Act: universality; comprehensiveness; portability; accessibility and public administration. We are a non-partisan public interest activist coalition and network.
To this end, we empower the members of our constituent organizations to become actively engaged in the making of public policy on matters related to our public health care system and healthy communities. We seek to provide to member organizations and the broader public ongoing information about our health care system and its programs and services, and to protect our public health system from threats such as cuts, delisting and privatization. Through public education and support for public debate, we contribute to the maintenance and extension of a system of checks and balances that is essential to good decision-making. We are an extremely collaborative organization, actively working with others to share resources and information.
Who We Are
The Ontario Health Coalition is comprised of a Board of Directors, committees of the Board as approved in the Coalition’s annual Action Plan, Local Coalitions, member organizations and individual members. Currently the Ontario Health Coalition represents more than 400 member organizations and a network of Local Health Coalitions and individual members. Our members include: seniors’ groups; patients’ organizations; unions; nurses and health professionals’ organizations; physicians and physician organizations that support the public health system; non-profit community agencies; ethnic and cultural organizations; residents’ and family councils; retirees; poverty and equality-seeking groups; women’s organizations, and others.
[1] See: http://www.healthsystemfacts.com/Client/OHA/HSF_LP4W_LND_WebStation.nsf/page/Average+Number+of+Inpatients+on+Any+Given+Day+Ontario
[2] Ontario Hospital Association at http://www.healthsystemfacts.com/Client/OHA/HSF_LP4W_LND_WebStation.nsf/page/Beds+staffed+and+in+operation+Ontario+1990+to+large
[5] See: Forster, A.J. et al “The Effect of Hospital Occupancy on Emergency Department Length of Stay and Patient Disposition” Academic Emergency Medicine, 2003; CIHI “Understanding Emergency Department Wait Times”; B.H.Rowe et al., “Frequency, Determinants, and Impact of Overcrowding in Emergency Departments in Canada” 2006; OHA, OMA, MOHLTC, “Improving Access to Emergency Care: Addressing System Issues” 2006.
[8] Wahl, Judith, Advocacy Centre for the Elderly. “ALC, Hospital Discharge, Long Term Care and Retirement Home – What Happened to the Law and Ethics?” Power Point presentation 2011.
To view submissions from our local coalitions, please click here.























HAMILTON










WINDSOR






THUNDER BAY








SAULT STE. MARIE




OTTAWA

